Thanks @ilivesunshine I had not seen this, it does not sound good news to me.
Look after yourself
Im absolutely horrified to read that article- cant quite get my thoughts together on it apart from feeling horrified! Thank you for posting
I’m adding my voice to this conversation of feeling horrified @ilivesunshine, @Erica and @judesadventures . How can this be???
You’re MORE likely to get Covid again if you take Paxlovid
Hi @Ted369 more bad news.
No I had not read this either, very interesting read ,one that the team @BloodCancerUK will be on to ,I am sure .
They published an update last week on the latest info on Evushield which was surprising!
https://l.facebook.com/l.php?u=https%3A%2F%2Fbloodcancer.org.uk%2Fnews%2Fevusheld-does-it-work-against-omicron%2F%3Ffbclid%3DIwAR3gmWC1_9j2CE8biNAFjeqDIqUYxoN8MG5LFuh0--x2Yj3IQqVG1tjOmSI&h=AT3rwZpuO-GwhSKzeNFBaS8qwyP41ImWVM3MWJ5gKmN1YuqAJW-YfXpN6xC6F_g5okIHzBnptMbVwRt_brsFQH7NhYV1YUGYrRQmEKrQHOZiiIvnqU6gODL_qfl31fE&s=1Soddx
In case you haven’t seen that update.
Jules
How complicated it all is!
Hi all, hope you’re all doing okay - we know the uncertainty around this is really hard.
NICE have published their draft guidance on which post-exposure Covid treatments to recommend or not recommend for use. NICE’s guidance must be followed by the NHS.
In their draft guidance, NICE have concluded that the following treatments are not cost effective:
- casirivimab plus imdevimab
- molnupiravir
- remdesivir
- sotrovimab
- Evusheld (used as post-exposure)
However, NICE have decided that, in the community setting, Paxlovid should remain in use, and tocilizumab should remain in use for hospitalised patients on supplemental oxygen. There is no treatment recommended for use for hospitalised patients not on supplemental oxygen. But for those patients who are hospitalised with Covid and aren’t yet on oxygen, there are non-Covid-specific treatments that are given, like corticosteroids.
NICE’s decisions around this have been based on a cost-effectiveness analysis which took into account: 1) hospitalisation rates, (2) time to discharge from hospital, (3) Long Covid costs, (4) administrative costs, and (5) hospitalisation costs.
It’s important to note that this is draft guidance and does not change policy until final guidance is issued in the spring. NICE will meet at the end of January to consider any rebuttals (including from patient support organisations). They will then produce and disseminate final guidance in or around March.
Patients will still be offered the current treatments until supplies run out. It is therefore likely that patients will continue to have access to all treatments over the winter period.
We totally understand that the uncertainty around this will be difficult for many people in the blood cancer community. Please be assured, that we are working hard to amplify the issues and concerns of the blood cancer community to the decision makers within the government. Blood Cancer UK are official stakeholders in the NICE appraisal, so we have the opportunity to comment on NICE’s draft guidance and decision. In our initial submission, we explained the Paxlovid has a lot of drug interactions with some treatments commonly given to people as part of their blood cancer care. We also explained that their decision should take into account the range of benefits provided by Covid treatments that aren’t captured solely by clinical efficacy data (like hospitalisation rate, for example).
We will continue to argue that there should be an alternative treatment available for people who cannot take Paxlovid due to drug interactions. It’s important to us that NICE understands that it can be harmful for people with blood cancer to stop taking treatments they need for their cancer care. NICE appreciates our input because the patient experience is important to them, so we hope that they’ll carefully consider our comments. There are dozens of other patient support organisations who will also be commenting on their draft guidance, including Anthony Nolan, Leukaemia Care, Leukaemia UK, Chronic lymphocytic leukaemia (CLL) Support, and Lymphoma Action. We all worked together on our original submission to NICE and will be sending separate comments to NICE to maximise our impact and ensure they understand that this is an issue that’s important to our community.
You may find it useful to read through our webpage here, which we are continually reviewing and updating: Antibody and antiviral treatments for people with blood cancer.
If you’re worried by this news, you may find it useful to talk to your haematology team/GP about a plan for if this guidance is approved in the spring, to make sure you’re aware which treatments you’re eligible for in the event of testing positive for Covid.
Please be assured that we will continue to update the blood cancer community as we learn more.
If any of you want to talk any of this through, we’re only a phone call or an email away, so please don’t hesitate to get in touch.
Take care all and remember we’re here if there’s anything we can do to support you.
I am worried now. I took Paxlovid when i caught covid. I have been merrily going here there and everywhere thinking i would be well protected after catching it. Now i read this. Is there no end to it!
Hi @Ted369 @ilivesunshine the way in which the article is titled is a bit misleading.
Paxlovid rebound doesn’t mean a new infection of covid, it’s a recurrence of symptoms or a new positive viral test after having tested negative. It’s an American document but this puts it quite well - COVID-19 Rebound After Paxlovid Treatment (cdc.gov)
”Paxlovid continues to be recommended for early stage treatment of mild to moderate COVID-19 among persons at high risk for progression to severe disease. Paxlovid treatment helps prevent hospitalization and death due to COVID-19. COVID-19 rebound has been reported to occur between 2 and 8 days after initial recovery and is characterized by a recurrence of COVID-19 symptoms or a new positive viral test after having tested negative. A brief return of symptoms may be part of the natural history of SARS-CoV-2 (the virus that causes COVID-19) infection in some persons, independent of treatment with Paxlovid and regardless of vaccination status"
While there’s evidence of some people experiencing a ‘rebound’ after taking Paxlovid, the drug also significantly reduces the chances of hospitalisation and death and is therefore an important defence against adverse health outcomes from the virus. Our health information team are going to be producing some content around Paxlovid and Paxlovid rebound soon so I’ll add it here when it’s published.
We’re only at the end of the phone if anyone wants to talk this through further, and as always, don’t hesitate to reach out to your healthcare team if you have any concerns.
Thank you @Alice_BloodCancerUK for this helpful information. That’s to some extent reassuring that the change won’t come into effect until after the winter as long as supplies don’t run out.
Saw this last week Erica and was concerned enough to look further.
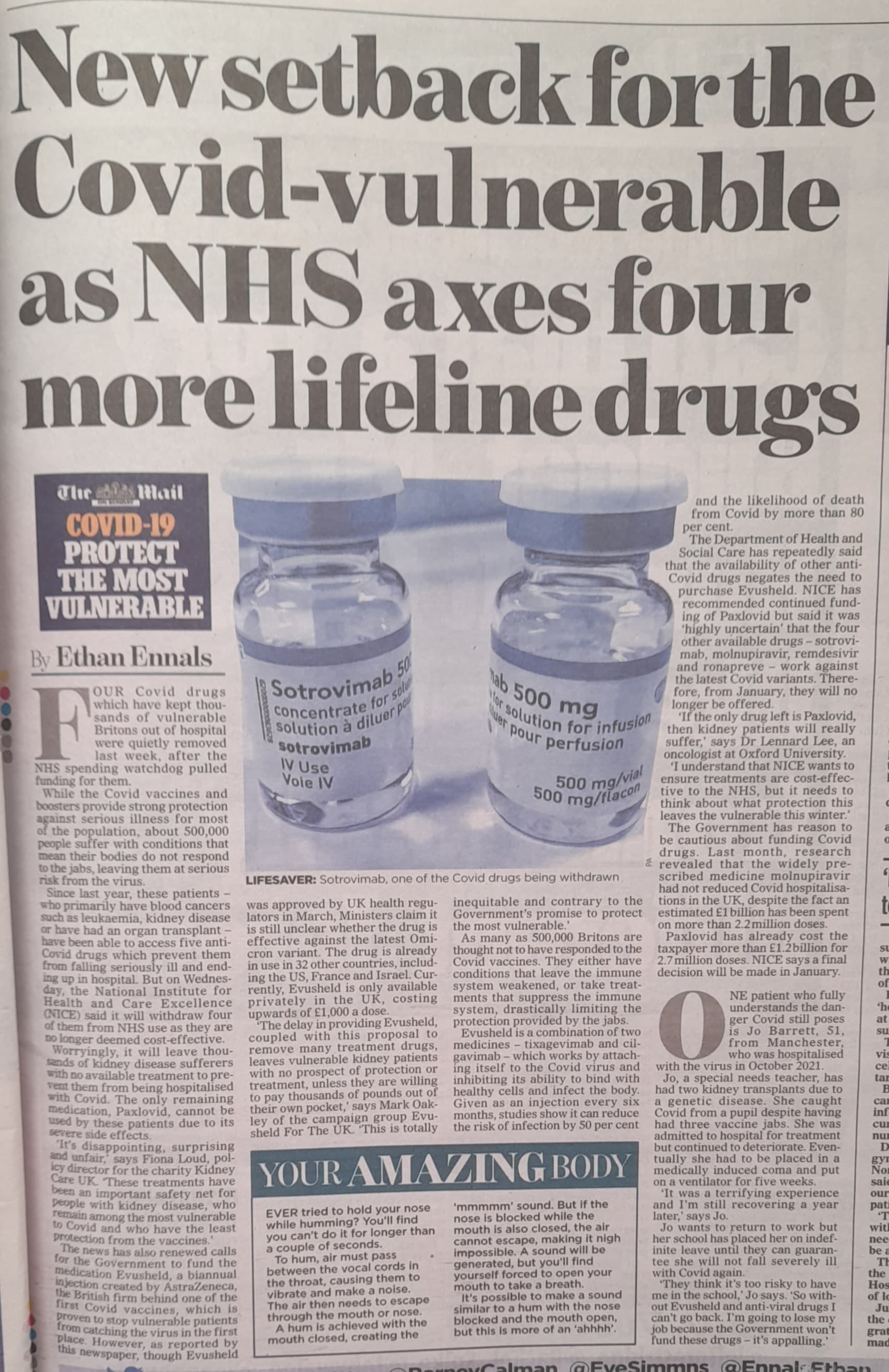
The four monoclonal antibody treatments have been withdrawn because they are not considered effective against Omicron.
The remaining ones are, it. seems only available IF we are hospitalised.
Not a good outlook at all.
Alice x
This is good to know and thanks for sharing. My husband had covid around three weeks ago. Although he is better than he was he still has cold type symptoms. Could this be rebound symptoms? ….he was given pavlovid
Thank you, Alice_BloodCancerUK and BCUK generally, for making the case on this for BC patients. One particular issue concerns me. I checked on the drug interactions for pavloxid (proposed to be the only treatment on offer in the community). I found that several drugs prescribed for control of Chronic lymphocytic leukaemia (CLL), including venetoclax and ibrutinib (probably also it’s cousin acalbrutinib, which I take) have interactions with pavlovid which could be contraindications for use.
While there are alternatives available, clinicians deciding on treatment can chose one without such interactions (eg molnupiravir). Even if those alternatives may not be so effective gejnerally, they might be the best option for BC patients taking medication interacting with pavloxid. Removing those alternatives would remove that choice.
If this makes sense, perhaps this could be noted in the representation BCUK makes to NICE on this?
Just wanted to add this here as promised - Paxlovid rebound - what we know | Blood Cancer UK
Please be assured Ben, that this is being included in our comments to NICE. If you want to chat anything through, please do give us a call on 0808 2080 888.
An interesting read on Twitter yesterday about a meeting between the Science and Technology Committee and Health and Social Care Committe with regard to anti virrals and Evusheld. They stated Paxlovid and molnupiravir were purchased under emergency provisions and were not reliant on the specific spike protein and there was no mention on stopping them. They did say some others had proved ineffective and so most countries had discontinued to use them.
Evesheld they said did relate to the specific spike protein and was now proved to be less effective. they said Canada and the USA were making patients aware that they would not have the cover they were expecting.
I do think we need to look beyond sensational headlines and look at the reasons and source of the information before panicking. Some headlines are very missleading.